|
|

 |
|
NeuroAIDS Vol. 4, No. 3, March 2001
|
Meningitis in HIV-positive patients
William G. Powderly, MD,
FRCPI1
1Professor of
Medicine, Chief, Division of Infectious Diseases, Department of Medicine,
Washington University School of Medicine, 660 South Euclid Ave., Campus
Box 8051, St. Louis, MO 63110
E-mail: wpowderl@imgate.wustl.edu
Keywords:
meningitis, tuberculosis, cryptococcosis
|
| Meningitis in patients with HIV infection is almost always infectious
in origin. Two opportunistic pathogens stand out as important problems in
patients with AIDS - Cryptococcus neoformans and Mycobacterium
tuberculosis, and together they account for about ¾ of the cases of
meningitis. The rates of cryptococcal meningitis have been decreasing in
the Western world with the introduction of effective suppressive therapy,
especially fluconazole, and the introduction of effective treatment for
HIV itself, with the consequent improvement in immune function. However,
in developing countries, both tuberculosis and cryptococcosis remain among
the most common and important causes of morbidity and mortality in
patients with AIDS. |
|
The cardinal clinical consequence of progressive infection with HIV is
the development of opportunistic infections (and to a lesser extent,
malignancies) as a consequence of progressive loss of immune function.
Although there are many potential pathogens that can complicate AIDS, in
most circumstances only a very limited number affect the brain. Meningeal
involvement can potentially complicate any opportunistic infection of the
brain; meningitis may also complicate primary infection with HIV itself.
However, two pathogens in particular, Cryptococcus neoformans and
Mycobacterium tuberculosis must always be considered when
evaluating meningitis in HIV-infected patients, because of the frequency
of infection, and the potential morbidity they
cause. |
|
Infection with C. neoformans is the most common systemic fungal
infection in patients infected with HIV and the most common cause of
meningitis (1).
About 5% of HIV-infected patients in the Western World develop
disseminated cryptococcosis (2)(3)(4);
the disease occurs in 20-30% of patients in other parts of the world such
as in sub-Saharan Africa, and Thailand. C. neoformans is found
worldwide as a soil organism; it is an encapsulated yeast measuring 4-6 um
with a surrounding polysaccharide capsule ranging in size from 1 to over
30 um. Two varieties, distinguishable by serology, exist - C.
neoformans var. neoformans (serotypes A and D) and C.
neoformans var. gatti (serotypes B and C). Virtually all
HIV-associated infection is caused by C. neoformans var.
neoformans (5).
It is unclear whether cryptococcal infection represents acute primary
infection or reactivation of previously dormant disease.
It is postulated that initial infection occurs via inhalation of the
basidiospores or unencapsulated forms leading to subsequent colonization
of the airways and subsequent respiratory infection (6).
Pulmonary macrophages are critically involved in control of the yeast (7),
and complement mediated phagocytosis appears to be the primary initial
defense against cryptococcal invasion (8).
Other host-yeast interactions including CD4+ and CD8+ T-cells, as well as cytokines (such as
gamma interferon, tumor necrosis factor alpha, IL-10 and 1l-12) also
appear to be important (9)(10).
In murine models, both CD4+ and
CD8+ T-cells are required to inhibit
cryptococcosis, and cytokines seem to be important in limiting
dissemination (10).
Thus, the defects in cell-mediated immunity characteristic of progressive
HIV infection can be seen to readily increase the risk of disseminated
cryptococcal infection.
The role of humoral immunity in control of cryptococcal infections is
less certain. A recent case-control study (11)
suggested an association between reduced expression of certain
immunoglobulin subsets and cryptococcal meningitis in HIV-infected
patients. In vitro studies of antibodies to the soluble capsular
polysaccharide of C. neoformans reveal enhanced phagocytosis,
increased fungicidal activity of leukocytes, and increased fungistatic
activity of natural killer cells (12).
The most common presentation of cryptococcosis is a subacute meningitis
or meningoencephalitis with fever, malaise and headache. Symptoms are
usually present for 2-4 weeks before diagnosis. Classic meningeal symptoms
and signs (such as neck stiffness or photophobia) occur in only about a
quarter to a third of patients(13).
Patients may present with encephalopathic symptoms such as lethargy,
altered mentation, personality changes and memory loss. Analysis of the
cerebrospinal fluid (CSF) usually shows a mildly elevated serum protein,
normal or slightly low glucose, and a lymphocytic pleocytosis. A minimal
inflammatory response characterized by less than 10
lymphocytes/mm3 CSF is seen in approximately 55% of cases (14).
As many as ¼ of HIV-positive patients presenting with cryptococcal
meningitis have normal CSF findings. Therefore, findings of an apparently
normal CSF should not exclude the possibility of cryptococcal infection.
India ink staining of the CSF will usually reveal the yeast. Cryptococcal
antigen is almost invariably detectable in the CSF. The opening pressure
in the CSF is elevated in a majority of patients.
|

|
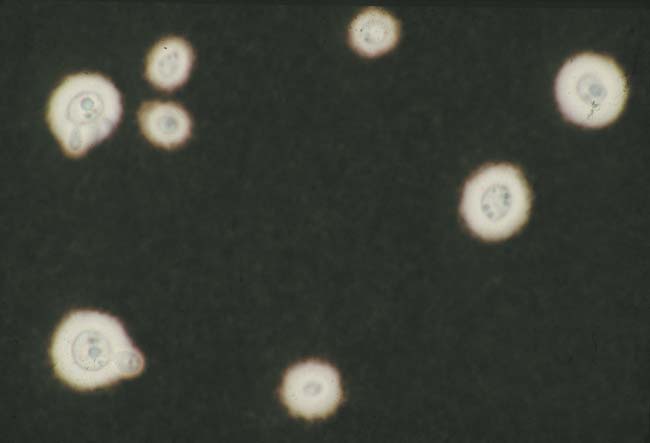
Figure 1 (Enlarge):
India Ink stain of CSF showing encapsulated yeast
|
Infection with C. neoformans can involve sites other than the
meninges. In patients with AIDS, dissemination is common and pulmonary
presentations such as cough, dyspnea or abnormal chest radiographs may be
the initial finding. Many patients have positive blood cultures. Skin
involvement is common; several types of skin lesions have been described
but the most common form is that resembling molluscum contagiosum.
|

|
Figure 2 (Enlarge):
Cutaneous lesions of disseminated cryptococcosis
|
The latex agglutination test for cryptococcal polysaccharide antigen in
the serum is highly sensitive and specific in the diagnosis of infection
with C. neoformans and a positive serum cryptococcal antigen titer
of greater than 1:8 is as presumptive evidence of cryptococcal infection.
Such patients should be evaluated for possible meningeal involvement.
Culture of C. neoformans from any body site should also be regarded
as significant and is an indication for further evaluation and initiation
of therapy.
|

|
Figure 3 (Enlarge):
GMS stain of brain showing invasive cryptococcosis
|
Untreated, cryptococcal
meningitis is fatal. In patients with AIDS, amphotericin B (0.7 mg/kg IV)
given for 2 weeks followed by fluconazole 400 mg PO for a further 8 weeks
is associated with the best outcome to date in prospective trials with a
mortality of less than 10% and a mycologic response of approximately 70%
(15)(16).
This regimen is also reasonable for treatment of meningitis in other
circumstances. Concomitant use of flucytosine, 100 mg/kg/day in four
divided doses, with amphotericin B may be considered. Flucytosine does not
improve immediate outcome, but may decrease the risk of relapse. The
combination of fluconazole, 400-800 mg /day with flucytosine and liposomal
formulations of amphotericin B are options for patients unable to tolerate
the usual formulation of amphotericin B (16).
Clinical deterioration in patients with meningitis may be due to
increased intracranial pressure, which may be diagnosed by a raised
opening pressure of the CSF. A recent study in patients with AIDS showed a
strong correlation between mortality in the first two weeks after
diagnosis, and the baseline opening pressure (17).
All patients with cryptococcal meningitis should have the opening pressure
measured when a lumbar puncture is performed, and strong consideration
should be given to reducing such pressure (by repeated lumbar punctures, a
lumbar drain or a shunt) if the opening pressure is high (>25 cm of
water).
Cryptococcal meningitis in AIDS requires lifelong suppressive therapy
unless the immunosuppression is reversed (16)(18).
Fluconazole, 200 mg daily, is the suppressive treatment of choice.
Fluconazole, in dosages ranging from 400 mg weekly to 200 mg daily, and
itraconazole, 100 mg twice daily, are very effective in preventing
invasive cryptococcal infections, especially in HIV-positive patients with
CD4 counts < 50-100 cells/mm3. (16)(19)
However, because of the relative infrequency of invasive fungal
infections, antifungal prophylaxis does not prolong life and is not
routinely recommended.
Other fungi rarely involve the meninges. Histoplasma capsulatum
meningitis can occasionally be an additional feature of disseminated
histoplasmosis. Candida species may also rarely cause meningitis.
Although mucosal candidiasis is very commonly a feature of HIV infection,
systemic candidiasis is rare and usually is a very late complication of
AIDS. Neutropenic patients and those using intravenous drugs are at
greater risk for invasive candidiasis, including candida meningitis. The
clinical features, and CSF findings are similar to cryptococcal
infection. |
|
Bacterial Infection (and other causes of
meningitis) |
|
Acute bacterial meningitis is an infrequent complication of HIV
infection. HIV-positive patients are at considerable increased risk for
pneumococcal infection (20).
However, pneumonia is the most common manifestation of this
predisposition, and although bacteremia is common, meningitis is not
commonly seen in the developed world. In contrast, bacterial meningitis is
much more common in HIV-infected patients in the developing world (1)(21).
The limited available data suggests that HIV infected patients are also at
slightly increased risk for invasive infections with Neisseria
meningitidis compared to the general population; however meningococcal
meningitis and septicemia remain infrequent. Neurosyphilis can also
complicate HIV infection. Central nervous system involvement in syphilis
may occur at any time after initial infection. In particular, syphilitic
meningitis may be seen within the first few weeks of infection or as a
primary presenting symptom. Meningeal and meningovascular involvement may
be suggested by changes in mental status, auditory or other cranial nerve
dysfunction, ocular abnormalities, signs of meningeal irritation
(meningismus), or stroke. CSF findings consistent with neurosyphilis
include elevated protein and elevated white blood cell count. A reactive
VDRL test on CSF is very specific for neurosyphilis but quite insensitive,
so clinical judgment must be used in making the diagnosis. Treatment of
choice for neurosyphilis is intravenous administration of aqueous
crystalline penicillin-G (12 to 24 million units) daily for 14 days.
Ceftriaxone may be an alternative (22).
The most important bacterial cause of meningitis in patients with AIDS
is tuberculosis (23).
Worldwide, tuberculosis is the most common opportunistic complication of
HIV infections and accounts for considerable morbidity. In the developed
world, there is considerable overlap among groups at high risk for TB and
HIV including those who are homeless, housed in institutions, injection
drug users, or living in urban areas where TB rates are high. In urban
areas where coinfection with TB and HIV is more common, there is also an
increased risk of acquisition of multiple-drug-resistant TB (MDR TB),
particularly among individuals previously treated with antimycobacterial
drugs.
The clinical manifestations of TB depend in part on the degree of
immunosuppression in the patient. When the patients are still relatively
immunocompetent, with CD4 lymphocyte counts > 200 cell/mm3 ,
pulmonary disease is most common. However, disseminated infection is more
likely to ensue with more advanced immunodeficiency. The sites most
frequently involved are the central nervous system (tuberculous
meningitis), the reticuloendothelial system (lymph nodes, spleen, liver,
bone marrow), or bone (vertebral bodies). However, virtually any other
organ can be infected during hematogenous dissemination. Tuberculous
meningitis may present clinically with fever, headache, mental-status
changes, or focal neurologic deficits. Analysis of the cerebrospinal fluid
usually shows an elevated serum protein, low glucose, and a lymphocytic
pleocytosis. Identification of the organism in the CSF is unusual although
cultures are typically positive within 2-3 weeks. Blood cultures may also
be positive, especially in the setting of disseminated infection. CT or
MRI scans of patients with tuberculous meningitis may show parenchymal
mass lesions (tuberculomas); there are conflicting data on the prevalence
of tuberculomas and other pathological changes that represent an
inflammatory response in HIV-infected patients (24)(25).
Untreated, tuberculous meningitis progresses relentlessly and is
uniformly fatal. Treatment of tuberculosis requires use of an adequate
number of active antituberculous drugs for a prolonged duration. Treatment
should be guided by antimycobacterial drug-susceptibility testing. Initial
isolates and isolates recovered from those who relapse or for whom therapy
fails should be tested for susceptibility to antituberculous drugs. In
HIV-positive patients, issues of therapy are also complicated by the
potential requirement for antiretroviral therapy. Many of the more potent
antiviral agents, such as the protease inhibitors and non-nucleoside
reverse transcriptase inhibitors have significant interactions with
rifamycins, which are critically important in the treatment of
tuberculosis (26).
Concomitant usage of potent antiretroviral therapy and anti-tuberculous
therapy requires expert management and should follow published guidelines
(26)
(27).
Management of tuberculosis is further complicated by the emergence of
resistance to treatment as a significant factor. In 1998, 8% of TB
isolates recovered from patients in the United States were resistant to at
least isoniazid, and 1.1% were resistant to at least isoniazid and
rifampin (28).
Development of resistance has been associated with poor adherence to
therapy, failure to recognize drug resistance leading to a delay in
initiation of appropriate treatment, and the use of ineffective treatment
regimens.
Initial therapy for uncomplicated TB in whom potent antiretroviral
therapy is not started should include at least four drugs: isoniazid,
rifampin, pyrazinamide, and either ethambutol or streptomycin (23)(29).
Tuberculous meningitis should be treated for at least 12 months. The role
of concomitant corticosteroids is uncertain (30).
Although some studies suggest that steroids may reduce acute mortality,
especially in children, there are limited data available on their use in
HIV-infected patients.
Unusual clinical manifestations have also been described in patients
receiving potent antiretroviral therapy. In the first few months after
starting antiretroviral therapy, patients may experience apparent
worsening of their tuberculosis with increased fever, pleural effusions,
enlarging lymph nodes (especially mediastinal). In patients with
meningitis, cerebritis and space-occupying lesions on scans has also been
described. This paradoxical worsening is probably immune-mediated, does
not imply failure of anti-TB treatment, and may respond to
corticosteroids.
Other causes of meningitis
Opportunistic viral meningitis is rare. In contrast, meningitis can be
a presentation of acute infection with HIV itself (31).
The clinical manifestations of symptomatic primary HIV infection are
myriad and most often include the acute onset of fever, generalized
lymphadenopathy, pharyngitis, erythematous maculopapular rash. Headache is
common and probably represents meningeal involvement in many cases.
However it is rarely severe enough to prompt evaluation that includes a
lumbar puncture. Aseptic meningitis with a lymphocytic pleocytosis is most
commonly seen when CSF is analyzed. More severe neurologic manifestations
including encephalitis, the Guillain-Barré syndrome, facial palsy, cauda
equina syndrome, brachial neuritis, and peripheral neuropathy may occur,
demonstrating the neurotropism of HIV. These manifestations usually
recover completely as the acute syndrome resolves.
One final consideration in meningitis in patients with HIV infection is
that it might be drug induced. Several cases of aseptic meningitis due to
trimethoprim/sulfamethoxazole have been described (32).
The presentation is one of acute meningitis with lymphocytic pleocytosis
on CSF analysis. Resolution is prompt when the drug is
stopped. |
|
Meningitis in patients with HIV disease is most frequently due to
opportunistic infections. Thus, predictions center on the likelihood of
controlling opportunistic infection. The best way to prevent opportunistic
infections is to give effective antiretroviral therapy - the future
epidemiology of opportunistic infections is inextricably linked with the
effectiveness of future antiretroviral treatment (33). |
|
(1) Hakim JG, Gangaidzo IT, Heyderman RS, et al.
Impact of HIV infection on meningitis in Harare, Zimbabwe: a prospective
study of 406 predominantly adult patients. AIDS. 2000; 14:1401-7. Medline
(2) Currie BP, Casadevall A. Estimation of the prevalence
of cryptococcal infection among patients infected with the human
immunodeficiency virus in New York City. Clin Infect Dis 19:1029, 1994. Medline
(3) Pinner RW, Hajjeh RA, Powderly WG. Prospects for
preventing cryptococcosis in persons infected with human immunodeficiency
virus. Clin Infect Dis 21(Suppl 1):S103, 1995. Medline
(4) Hajjeh RA, Conn LA, Stephens DS, et al.
Cryptococcosis: population-based multistate active surveillance and risk
factor in human immunodeficiency virus-infected persons.Cryptococcal
Active Surveillance Group. J Infect Dis 1999 ;179:449-54. Medline
(5) Rinaldi MG, Drutz DJ, Howell A, Sande MA, Wofsy CB,
Hadley WK. Serotypes of Cryptococcus neoformans in patients with AIDS. J
Infect Dis 1986; 153:642. Medline
(6) Levitz SM. The ecology of Cryptococcus neoformans and
the epidemiology of cryptococcosis. Rev Infect Dis 1991; 13: 1163-1169. Medline
(7) Perfect JR, Granger DL, Durack DT. Effects of
antifungal agents and gamma interferon on macrophage cytotoxicity for
fungi and tumor cells. J Infect Dis 1987;156:316-323. Medline
(8) Kwon-Chung KJ, Kozel TR, Edman JC, et al. Recent
advances in biology and immunology of Cryptococcus neoformans. J Med Vet
Mycol 1992; 30:133-142. Medline
(9) Huffnagle GB, Lipscomb MF. Cells and cytokines in
pulmonary cryptococcosis. Res Immunol 1998; 149:387-96. Medline
(10) Lortholary O, Improvisi L, Rayhane N, Gray F,
Fitting C, Cavaillon JM, Dromer F. Cytokine profiles of AIDS patients are
similar to those of mice with disseminated Cryptococcus neoformans
infection. Infect Immun 1999; 67:6314-20. Medline
(11) Fleuridor R, Lyles RH, Pirofski L. Quantitative and
qualitative differences in the serum antibody profiles of human
immunodeficiency virus-infected persons with and without Cryptococcus
neoformans meningitis. J Infect Dis. 1999; 180:1526-35. Medline
(12) Casadevall A. Antibody immunity and invasive fungal
infections. Infect Immun 1995; 63:4211-4218. Medline
(13) Chuck SL, Sande MA. Infections with Cryptococcus
neoformans in the acquired immunodeficiency syndrome. N Engl J Med 1989;
321:794-799. Medline
(14) Darras-Joly C, Chevret S, Wolff M, et al.
Cryptococcus neoformans infection in France: epidemiologic features of and
early prognostic parameters for 76 patients who were infected with human
immunodeficiency virus. Clin Infect Dis 1996;23:369-376. Medline
(15) van der Horst CM, Saag NS, Cloud GA, et al.
Treatment of cryptococcal meningitis associated with the acquired
immunodeficiency syndrome. National Institute of Allergy and Infectious
Diseases Mycoses Study Group and AIDS Clinical Trials Group. N Engl J Med
1997; 337:15-21. Medline
(16) Saag MS, Graybill RJ, Larsen RA, Pappas PG, Perfect
JR, Powderly WG, Sobel JD, Dismukes WE. Practice guidelines for the
management of cryptococcal disease. Infectious Diseases Society of
America. Clin Infect Dis 2000 ;30:710-8. Medline
(17) Graybill JR, Sobel J, Saag M, et al. Diagnosis and
management of increased intracranial pressure in patients with AIDS and
cryptococcal meningitis. The NIAID Mycoses Study Group and AIDS
Cooperative Treatment Groups. Clin Infect Dis 2000; 30:47-54. Medline
(18) Powderly WG, Saag MS, Cloud GA, et al. A controlled
trial of fluconazole or amphotericin B to prevent relapse of cryptococcal
meningitis in patients with the acquired immunodeficiency syndrome. The
NIAID AIDS Clinical Trials Group and Mycoses Study Group. N Engl J Med
1992; 326:793-8. Medline
(19) Powderly WG, Finkelstein D, Feinberg J, et al. A
randomized trial comparing fluconazole with clotrimazole troches for the
prevention of fungal infections in patients with advanced human
immunodeficiency virus infection. NIAID AIDS Clinical Trials Group. New
Engl J Med 1995; 332:700-705. Medline
(20) Janoff EN, Breiman RF, Daley CL and Hopewell PC.
Pneumococcal disease during HIV infection. Epidemiologic, clinical, and
immunologic perspectives. Annals of Internal Medicine 1992; 117:314-324.
Medline
(21) Gordon SB, Walsh AL, Chaponda M, et al. Bacterial
meningitis in Malawian adults: pneumococcal disease is common, severe, and
seasonal. Clin Infect Dis. 2000; 31:53-7. Medline
(22) Marra CM, Boutin P, McArthur JC, et al. A pilot
study evaluating ceftriaxone and penicillin G as treatment agents for
neurosyphilis in human immunodeficiency virus-infected individuals. Clin
Infect Dis. 2000; 30:540-4. Medline
(23) Havlir DV, Barnes PF. Tuberculosis in patients with
human immunodeficiency virus infection. N Engl J Med. 1999; 340:367-73. Medline
(24) Dube MP, Holtom PD, Larsen RA. Tuberculous
meningitis in patients with and without human immunodeficiency virus
infection. Am J Med 1992; 93:520-4. Medline
(25) Katrak SM, Shembalkar PK, Bijwe SR, Bhandarkar LD.
The clinical, radiological and pathological profile of tuberculous
meningitis in patients with and without human immunodeficiency virus
infection. J Neurol Sci 2000; 181:118-26. Medline
(26) Centers for Disease Control and Prevention. Notice
to Readers: Updated Guidelines for the Use of Rifabutin or Rifampin for
the Treatment and Prevention of Tuberculosis Among HIV-Infected Patients
Taking Protease Inhibitors or Nonnucleoside Reverse Transcriptase
Inhibitors. Morb Mortal
Weekly Rep. 2000; 49:185.
(27) Centers for Disease Control and Prevention.
Prevention and Treatment of Tuberculosis Among Patients Infected with
Human Immunodeficiency Virus: Principles of Therapy and Revised
Recommendations. Morb Mortal
Weekly Rep. 1998; 47(RR20);1-51
(28) Centers for Disease Control and Prevention.
Progress Toward the Elimination of Tuberculosis -- United States, 1998.
Morb Mortal Weekly Rep. 1999; 48;732-736.
(29) Pozniak AL, Miller R, Ormerod LP. The treatment of
tuberculosis in HIV-infected persons. AIDS 1999; 13:435-45. Medline
(30) Prasad K, Volmink J, Menon GR. Steroids for
treating tuberculous meningitis (Cochrane review). Cochrane Database Syst
Rev. 2000:CD002244. Medline
(31) Schacker T, Collier AC, Hughes J, Shea T &
Corey L. Clinical and epidemiologic features of primary HIV infection. Ann
Intern Med 1996; 125:257-264. Medline
(32) Jurado R, Carpenter SL, Rimland D. Case reports:
trimethoprim-sulfamethoxazole-induced meningitis in patients with HIV
infection. Am J Med Sci. 1996; 312:27-9. Medline
(33) Powderly WG. Prophylaxis for opportunistic
infections in an era of effective antiretroviral therapy. Clin Inf Dis
2000; 31:597-601. Medline |
|
|
{kind=link}