|
|
|
| NeuroAIDS Vol. 1, No. 1, May 1998 |
| HIV quantification in the central nervous system |
| V. Soontornniyomkij and C. A. Wiley |
| University of Pittsburgh Medical Center, Division of Neuropathology, Pittsburgh, Pennsylvania, United States. |
| Address correspondence to: wiley@np.awing.upmc.edu |
Abstract
| ||||||||||||
![]() his article has two purposes: to review techniques that have been employed for assessment of CNS HIV burden to and address new quantitative RNA assays used to assess HIV load in body fluids and tissue homogenates.
his article has two purposes: to review techniques that have been employed for assessment of CNS HIV burden to and address new quantitative RNA assays used to assess HIV load in body fluids and tissue homogenates.
Introduction
Background
HIV-1 associated dementia complex (ADC) occurs in approximately one quarter of all terminally-ill AIDS patients. While the clinical manifestations of some CNS opportunistic diseases may mimic dementia, a causal relationship between HIV and ADC was first suggested in 1985 by Shaw, et al. Using Southern blot analysis and in situ hybridization (ISH), they detected HIV DNA and RNA in cerebral tissue from a small group of patients with ADC. In one patient, the abundance of viral DNA in the brain exceeded that found in spleen or lymph nodes (Shaw et al. 1985). In the same year, Levy, et al. and Ho, et al. successfully isolated HIV from the neural tissues and cerebrospinal fluid of patients with ADC by co-cultivation with peripheral blood mononuclear cells (Levy et al. 1985; Ho et al. 1985). Subsequent clinical-pathological studies have suggested that a chronic productive HIV-1 infection in the brain (i.e. HIV encephalitis) is the pathological substrate of ADC (Navia et al. 1986; Wiley and Achim 1994).
Gap in Knowledge
There is some ongoing controversy regarding the importance of CNS viral burden in mediating neurologic disease (Wiley and Achim 1994; Brew et al. 1995; Glass et al. 1995; Johnson et al. 1996). Previous studies on relationship between CNS viral burden and ADC have not yet reached agreement. Part of this controversy is attributed to the variety of detection techniques employed in different laboratories to assess HIV burden. Even using similar methods, different study groups often generate vastly different results. A reproducible quantitative assay that can be used in any laboratory is needed to permit ready cross-study comparisons. In addition, it is known that HIV infection is not uniformly distributed throughout the CNS, but is preferentially localized to certain anatomical regions (Kure et al. 1990; Brew et al. 1995). Therefore, the extent of CNS tissue sampling is also important, and may require a consensus guideline.
Techniques I
In situ hybridization
Data: ISH has been employed by several groups to detect HIV RNA in tissue sections. Shaw, et al. applied this technique on frozen cerebral sections and found positive signals in 4 of 15 brains from patients with ADC (Shaw et al. 1985). Numerous other groups have found varying numbers of HIV probe-labeled cells in autopsied brains. Initial attempts to quantify this signal employed counting cells and grains per cells. Recently, Haase, et al. applied isotopic ISH and quantitative image analysis to assess HIV RNA load in human lymphoid tissues (Haase et al. 1996). Similar technology has been applied to SIV infection in rhesus macaques where viral RNA loads in CNS tissue sections were determined by a 4-tiered scoring system derived from counting viral RNA-positive cells per tissue sectional area (Reinhart et al. 1997).
Conclusions: None of these semi-quantitative techniques have gained widespread acceptance or been compared between laboratories.
PCR-ISH and Reverse Transcriptase (RT) in situ PCR
Data: Studies using PCR-ISH technology from different laboratories have shown conflicting results. Nuovo, et al. showed that a number of HIV DNA-positive cells was increased by 10- to more than 100-fold, compared to the standard ISH method (Nuovo et al. 1994). In this study, significant proportions of neurons and astrocytes were shown to contain viral DNA and RNA, in addition to microglia/macrophages. Using a combination of PCR-ISH, RT-PCR-ISH, and fluorescent imunocytochemistry (ICC), Bagasra, et al. concluded that HIV also infected neurons, endothelial cells, astrocytes, and oligodendrocytes (Bagasra et al. 1996). In dorsal root ganglia, Brannagan, et al. detected HIV DNA and RNA in satellite cells and occasional neurons of HIV-infected patients with peripheral neuropathy (Brannagan III et al. 1997). In contrast to the studies mentioned above, Takahashi, et al. found no convincing evidence of HIV infection in neurons, oligodendrocytes, and endothelial cells by PCR-ISH, although HIV DNA was detected in fewer than 1% of astrocytes in sections with HIV encephalitic features (Takahashi et al. 1996).
Conclusions: Potentiality of PCR-ISH technology would allow HIV detection in tissue at the level of single copy of viral DNA and concomitantly to determine its cellular localization. However, clearly great variability exists between different laboratories using this technology. Orders of magnitude differences suggest it may be a long time, if ever, before a consensus on this technology is reached.
Immunocytochemistry
Data: Detection of HIV proteins on CNS tissue sections has been achieved by ICC with antibodies to gag proteins (p17 and p24) and to transmembrane envelope protein (gp41) (Wiley et al. 1986; Sinclair et al. 1994; Achim et al. 1994). Studies from Kure, et al. and Budka, et al. had shown that a monoclonal antibody to gp41 (Clone 41.1, Genetic Systems) was most sensitive on paraffin CNS sections, compared to antibodies to p17 and p24 (DuPont) (Kure et al. 1990; Budka 1990). Our own experience confirmed this observation.
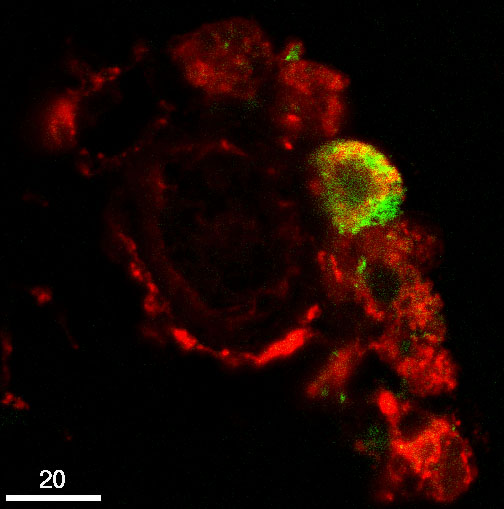
| Figure 1. Confocal microscopy of double immunofluorescent staining for RCA-1 (red) and HIV gp41 protein (green). At least one of perivascular RCA-1 stained macrophages is infected with HIV, as evidenced by co-localization of RCA-1 and gp41 (yellow). |
Specifically, ICC with avidin-biotin-peroxidase complex (ABC) method for gp41 (Genetic Systems) yielded many more positive cells than that for p24 (DAKO) on serial paraffin sections. Multinucleated giant cells, microglial nodules, and variable numbers of microglia and perivascular macrophages labeled intensely with the anti-gp41 antibody. Strangely, to date, no ICC has successfully detected the other portion of the envelope protein gp120 in fixed tissue (Budka 1990). Recently, a new signal amplification method was introduced into ICC protocols. This method amplifies signal via binding of tyramide to proteins near the site of peroxidase-labeled antibodies or strepavidin (von Wasielewski et al. 1997). Strappe, et al. reported a significant increase in sensitivity of ICC for p24 (DuPont) with tyramide signal amplification (TSA, DuPont) on paraffin brain sections. With microwave irradiation of brain sections in citrate buffer, the TSA method yielded higher staining intensity and up to 2-fold increases of the number of p24-positive foci, when compared to the ABC method. However, this study did not compare the sensitivity of TSA method for p24 to that of the ABC method for gp41 (Strappe et al. 1997).
Quantification of HIV-stained cells had been attempted in several studies. Vazeux, et al. assessed overall CNS viral load with 4-tiered estimation of the number of HIV-stained cells per section, and determination of the proportion of positive tissue blocks to all blocks examined in each case (Vazeux et al. 1987). Our group devised a scoring system for semi-quantification of gp41-stained cells (Genetic Systems) (Masliah et al. 1992). Three CNS regions (i.e. cortical gray matter, cerebral white matter, and deep gray matter) were assessed on paraffin sections taken from the mid-frontal gyrus and basal ganglia. We had applied this scoring system to determine the overall brain viral burden, and correlated brain viral load with histologic evidence of neocortical damage, clinical diagnosis of ADC, length of survival after AIDS diagnosis (Masliah et al. 1992; Wiley and Achim 1994; Soontornniyomkij et al. 1997). Glass, et al. also quantified gp41 immunostaining on paraffin sections of the mid-frontal gyrus and basal ganglia with a scoring system quite different from that developed by our group (Glass et al. 1995). Brew, et al. sampled brains and spinal cords systematically and extensively, and determined the proportion of p24-positive tissue sections in each case (Brew et al. 1995).
Conclusions: While the immunocytochemical semi-quantification of CNS HIV burden has shed some light on the pathogenesis of HIV encephalitis, several drawbacks are inherent in this technology. Numerous fixation parameters limit successful ICC on tissue sections, leading to false-negative and false-positive staining. Additionally, semi-quantification of morphology-based assessment (like ICC) requires extensive professional interpretation and would thus be expected to be difficult to replicate between laboratories.
Techniques II"
ELISA-based antigen capture assay
Data: Our group applied an ELISA-based antigen capture assay (ACA) (Coulter) to quantify HIV p24 protein in brain tissue homogenates (Achim et al. 1994). This quantitative technique was less sensitive than the semi-quantitative ICC for gp41 in detecting HIV proteins in brain tissue, possibly because of non-specific blocking proteins and lipids.
Conclusions: In the future the sensitivity of ELISA-based ACA may be increased by improvements in detection method (e.g. chemiluminescence) or higher affinity antibodies.
PCR and RT-PCR
Data: An assortment of PCR-based methods and quantitative analyses have been applied to assess CNS HIV load in different laboratories. Most previous studies were carried out on tissue from only one cerebral region (Boni et al. 1993;Sinclair et al. 1994; Johnson et al. 1996; An et al. 1996; Lazarini et al. 1997). Our group employed PCR on tissue from the mid-frontal cortex, white matter, and basal ganglia, and quantified HIV DNA using an enzyme oligonucleotide assay (Cellular Products) (Achim et al. 1994). We found HIV DNA was most abundant in the basal ganglia. Fujimura, et al. examined tissue from several brain regions by a quantitative PCR method, and found variable levels of HIV DNA in different regions (Fujimura and Bockstahler 1995). The viral levels in the hippocampus were 3-fold higher than those in the basal ganglia.
Conclusions: As different PCR and quantitative techniques were applied, several study groups have generated conflicting results. Limited tissue sampling may also contribute to misleading interpretation.
Quantitative HIV RNA assays
Data: Recently HIV has been quantified in plasma using a variety of highly-sensitive RNA assays based on either signal amplification (e.g., branched-DNA assay, Quantiplex HIV RNA, ChironCorporation) or template amplification (e.g., RT-PCR assay, Amplicor HIV-1 Monitor, Roche MolecularSystems, and nucleic acid sequence-based assay, NASBA HIV-1 RNA QT, Organon Teknika) (Schuurman et al. 1996). The Quantiplex assay has also been applied to lymphoid tissues (Haase et al. 1996; Harris et al. 1997). Recently, our group has employed both Quantiplex and Amplicor to determine the regional distribution of brain viral load in AIDS autopsies (Wiley et al. submitted 1997). We found a good correlation between these two techniques in quantitative performance. In addition, the HIV RNA load generally correlated well with HIV gp41 protein load assessed by our immunocytochemical scoring system.
Conclusions: Of the truly quantitative techniques, HIV RNA assays of tissue homogenates hold the greatest promise for objective cross-study comparisons.
Conclusions"
A variety of techniques to quantify HIV in the CNS have led to vastly different results in different laboratories. It is important to identify a reproducible quantitative assay that can be applied in any laboratory. Of the truly quantitative techniques, HIV RNA assays of tissue homogenates hold the greatest promise for objective cross-study comparisons. In addition, the extent of CNS tissue sampling is another issue that needs to be resolved. A consensus guideline for tissue sampling may be necessary. A wide range of studies on different patient populations can be compared systematically when the same reproducible technique and tissue sampling guideline are applied.
References
Achim CL, Wang R, Miners DK, Wiley CA (1994) Brain viral burden in HIV infection. J Neuropathol Exp Neurol 53: 284-94 Medline
An SF, Giometto B, Scaravilli F (1996) HIV-1 DNA in brains in AIDS and pre-AIDS: correlation with the stage of disease. Ann Neurol 40: 611-617 Medline
Bagasra O, Lavi E, Bobroski L, Khalili K, Pestaner JP, Tawadros R, Pomerantz RJ (1996) Cellular reservoirs of HIV-1 in the central nervous system of infected individuals: identification by the combination of in situ polymerase chain reaction and immunohistochemistry. AIDS 10: 573-85 Medline
Boni J, Emmerich BS, Leib SL, Wiestler OD, Schupbach J, Kleihues P (1993) PCR identification of HIV-1 DNA sequences in brain tissue of patients with AIDS encephalopathy. Neurology 43: 1813-7 Medline
Brannagan III TH, Nuovo GJ, Hays AP, Latov N (1997) Human immunodeficiency virus infection of dorsal root ganglion neurons detected by polymerase chain reaction in situ hybridization. Ann Neurol 42: 368-372 Medline
Brew BJ, Rosenblum M, Cronin K, Price RW (1995) AIDS dementia complex and HIV-1 brain infection: clinical-virological correlations [see comments]. Ann Neurol 38: 563-70 Medline
Budka H (1990) Human immunodeficiency virus (HIV) envelope and core proteins in CNS tissues of patients with the acquired immune deficiency syndrome (AIDS). Acta Neuropathol 79: 611-619 Medline
Fujimura RK, Bockstahler LE (1995) Polymerase chain reaction method for determining ratios of human immunodeficiency virus proviral DNA to cellular genomic DNA in brain tissues of HIV-infected patients. J Virol Methods 55: 309-25 Medline
Glass JD, Fedor H, Wesselingh SL, McArthur JC (1995) Immunocytochemical quantitation of human immunodeficiency virus in the brain: correlations with dementia. Ann Neurol 38: 755-762 Medline
Haase AT, Henry K, Zupancic M, Sedgewick G, Faust RA, Melroe H, Cavert W, Gebhard K, Staskus K, Zhang ZQ, Dailey PJ, Balfour HH, Jr., Erice A, Perelson AS (1996) Quantitative image analysis of HIV-1 infection in lymphoid tissue. Science 274: 985-9 Medline
Harris M, Patenaude P, Cooperburg P, Filipenko D, Thorne A, Raboud J, Rae S, Dailey P, Chernoff D, Todd J, Conway B, Montaner JSG, INCAS Study Group (1997) Correlation of virus load in plasma and lymph node tissue in human immunodeficiency virus infection. J Infect Dis 176: 1388-1392 Medline
Ho DD, Rota TR, Schooley R, Kaplan JC, Allan JD, Groopman JE, Resnick L, Felsenstein D, Andrews CA, Hirsch M (1985) Isolation of HTLV-III from cerebrospinal fluid and neural tissues of patients with neurologic syndromes related to the acquired immunodeficiency syndrome. N Engl J Med 313: 1493-1497 Medline
Johnson RT, Glass JD, McArthur JC, Chesebro BW (1996) Quantitation of human immunodeficiency virus in brains of demented and nondemented patients with acquired immunodeficiency syndrome. Ann Neurol 39: 392-395 Medline
Kure K, Weidenheim KM, Lyman WD, Dickson DW (1990) Morphology and distribution of HIV-1 gp41-positive microglia in subacute AIDS encephalitis. Pattern of involvement resembling a multisystem degeneration. Acta Neuropathol (Berl). 80: 393-400 Medline
Lazarini F, Seilhean D, Rosenblum O, Suarez S, Conquy L, Uchihara T, Sazdovitch V, Mokhtari K, Boussin F, Katlama C, Bricaire F, Duyckaerts C, Hauw JJ (1997) Human immunodeficiency virus type 1 DNA and RNA load in brains of demented and nondemented patients with acquired immunodeficiency syndrome. J Neurovirol 3: 299-303 Medline
Levy JA, Shimabukuro J, Hollander H, Mills J, Kaminsky L (1985) Isolation of AIDS-associated retroviruses from cerebrospinal fluid and brain of patients with neurological symptoms. Lancet 2: 586-588 Medline
Masliah E, Achim CL, Ge N, DeTeresa R, Terry RD, Wiley CA (1992) Spectrum of human immunodeficiency virus-associated neocortical damage. Ann Neurol 32: 321-9 Medline
Navia BA, Cho ES, Petito CK, Price RW (1986) The AIDS dementia complex: II. Neuropathology. Ann Neurol 19: 525-535 Medline
Nuovo GJ, Gallery F, MacConnell P, Braun A (1994) In situ detection of polymerase chain reaction-amplified HIV-1 nucleic acids and tumor necrosis factor-alpha RNA in the central nervous system. Am J Pathol 144: 659-666 Medline
Reinhart TA, Rogan MJ, Huddleston D, Rausch DM, Eiden LE, Haase AT (1997) Simian immunodeficiency virus burden in tissues and cellular compartments during clinical latency and AIDS. J Infect Dis 176: 1198-1208 Medline
Schuurman R, Descamps D, Weverling GJ, Kaye S, Tijnagel J, Williams I, van Leeuwen R, Tedder R, Boucher CA, Brun-Vezinet F, Loveday C (1996) Multicenter comparison of three commercial methods for quantification of human immunodeficiency virus type 1 RNA in plasma. J Clin Microbiol 34: 3016-22 Medline
Shaw GM, Harper ME, Hahn BH, Epstein LG, Gajdusek DC, Price RW, Navia BA, Petito CK, O'Hara CJ, Groopman JE, et.al. (1985) HTLV-III infection in brains of children and adults with AIDS encephalopathy. Science 227: 177-182 Medline
Sinclair E, Gray F, Ciardi A, Scaravilli F (1994) Immunohistochemical changes and PCR detection of HIV provirus DNA in brains of asymptomatic HIV-positive patients. J Neuropathol Exp Neurol 53: 43-50 Medline
Soontornniyomkij V, Nieto-Rodriguez JA, Martinez AJ, Kingsley LA, Achim CL, Wiley CA (1997) Brain HIV burden and length of survival after AIDS diagnosis. Clin Neuropathol (in press)
Strappe PM, Wang TH, McKenzie CA, Lowrie S, Simmonds P, Bell JE (1997) Enhancement of immunohistochemical detection of HIV-1 p24 antigen in brain by tyramide signal amplification. J Virol Methods 67: 103-112 Medline
Takahashi K, Wesselingh SL, Griffin DE, McArthur JC, Johnson RT, Glass JD (1996) Localization of HIV-1 in human brain using polymerase chain reaction/in situ hybridization and immunocytochemistry. Ann Neurol 39: 705-11 Medline
Vazeux R, Brousse N, Jarry A, Henin D, Marche C, Vedrenne C, Mikol J, Wolff M, Michon C, Rozenbaum W (1987) AIDS subacute encephalitis. Identification of HIV-infected cells. Am J Pathol 126: 403-410 Medline
von Wasielewski R, Mengel M, Gignac S, Wilkens L, Werner M, Georgii A (1997) Tyramide amplification technique in routine immunohistochemistry. J Histochem Cytochem 45: 1455-1459 Medline
Wiley C, Schrier RD, Nelson JA, Lampert PW, Oldstone MB (1986) Cellular localization of human immunodeficiency virus infection within the brains of acquired immune deficiency syndrome patients. Proc Natl Acad Sci USA 83: 7089-7093 Medline
Wiley CA, Achim C (1994) Human immunodeficiency virus encephalitis is the pathological correlate of dementia in acquired immunodeficiency syndrome. Ann Neurol 36: 673-676 Medline
Wiley CA, Soontornniyomkij V, Radhakrishnan L, Masliah E, Mellors J, Hermann SA, Dailey P, Achim CL (1998) Distribution of brain HIV load in AIDS. Brain Pathology 8(2): 277-284 Medline
| Copyright Information | Site map |