|
|
|
| AIDScience Vol. 3, No. 13, July 2002 |
 |
| VaxGen: are there hints of race-based effects? |
| by Patricia Kahn* |
| From the IAVI Report, the newsletter of the International AIDS Vaccine Initiative. Address correspondence to: pkahn@iavi.org. Reprinted with permission from the IAVI Report. |
| For six intense days, scientists gathered in the Canadian Rockies for the annual Keystone conference on HIV Vaccine Development (28 March-4 April 2003, Banff, Alberta). This year’s agenda offered a typically broad range of themes, from new findings on viral escape in monkeys to studies grappling with the question of just which T-cell subsets are most important for fighting HIV and evaluating vaccine candidates. Here we present headline stories from three corporate players: VaxGen, which discussed results from its recently completed Phase III trial; Merck, with updates on its Phase I clinical trials and announcing a new partnership with Aventis Pasteur; and Wyeth-Aherst, describing a strategy that may improve the usefulness of DNA-based vaccines. Other conference topics will be covered in the next issue of the IAVI Report. |
| ||||||||||||||
![]() hilip Berman, developer of VaxGen’s gp120-based AIDSVAX® vaccine, gave a much-anticipated talk on the outcome of the company’s North America/Europe Phase III trial. It was the first presentation of the trial’s efficacy results to a scientific audience, following a 24 February webcast describing the initial analysis. At that time, VaxGen made the startling and highly controversial claim that, although the vaccine showed no efficacy across the whole cohort, it protected about two-thirds of African-American, Asian and mixed-race volunteers.
hilip Berman, developer of VaxGen’s gp120-based AIDSVAX® vaccine, gave a much-anticipated talk on the outcome of the company’s North America/Europe Phase III trial. It was the first presentation of the trial’s efficacy results to a scientific audience, following a 24 February webcast describing the initial analysis. At that time, VaxGen made the startling and highly controversial claim that, although the vaccine showed no efficacy across the whole cohort, it protected about two-thirds of African-American, Asian and mixed-race volunteers.
But outside researchers quickly discovered a key flaw in the statistical analysis, greatly weakening the company’s claim that the protection data showed high statistical significance. Nevertheless, VaxGen stood by its statement that the vaccine holds promise for this mélange of non-white racial subgroups, a conclusion they said was supported by unreleased data correlating protection in these subgroups with higher antibody levels.
Against this backdrop, Berman’s talk in Banff provided a first glimpse of these (and other) studies aimed at building a biologically plausible case for race-based efficacy. “Our hypothesis is still that protection depends on the amount of antibody and the strain of virus,” he said. He also discussed possible gender-based differences in protection. Slides from the talk are available on VaxGen’s website.
|
But to HIV sequence expert Bette Korber (Los Alamos National Laboratory), the data showed no more than “a hint of a hint of an effect.” Further dimming the vaccine’s prospects, Berman said there is no evidence of reduced viral load or slower CD4 T-cell decline in vaccinees who became infected.
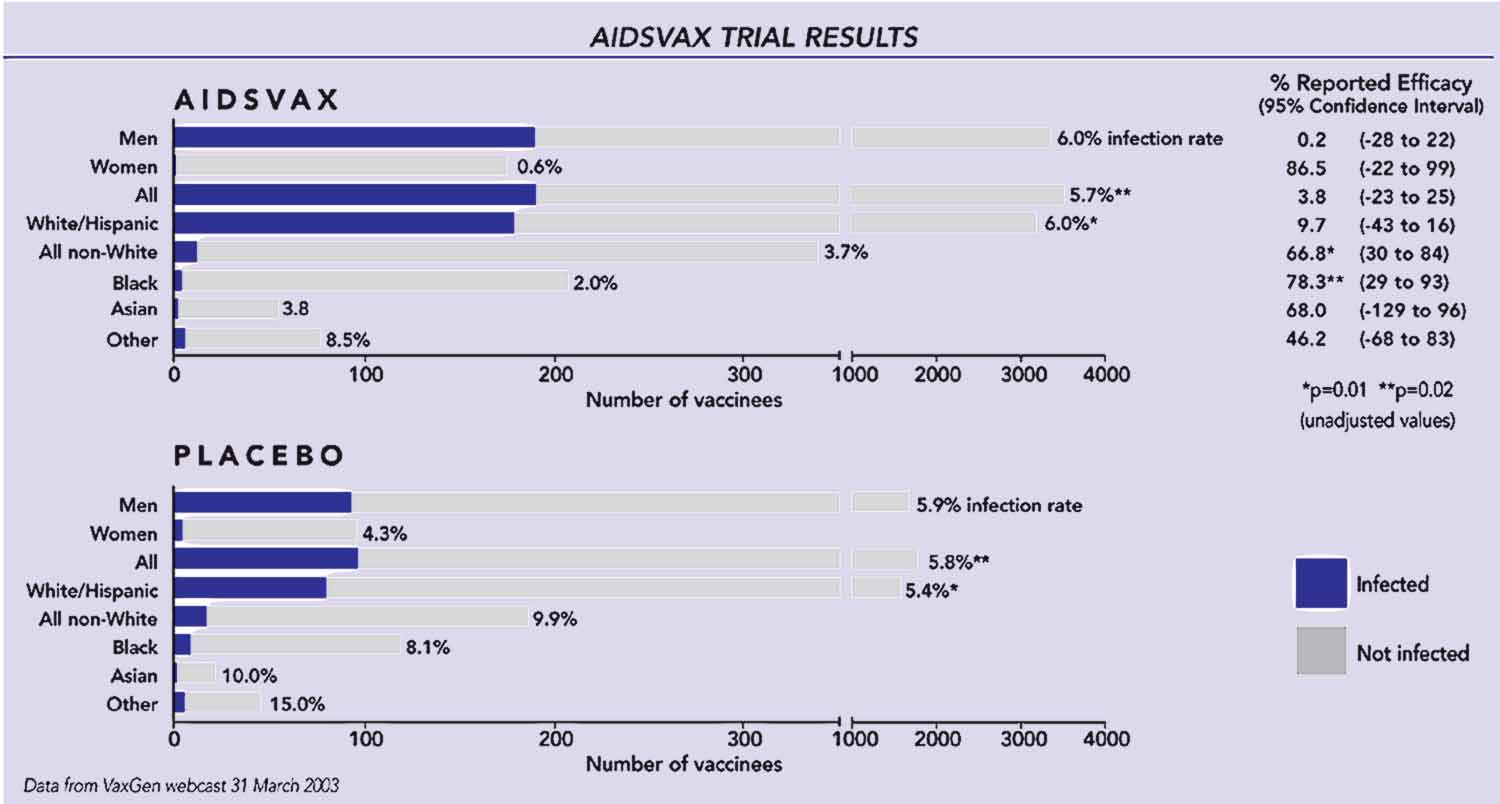
Trial results and racial subgroups
He began by reviewing the study’s main results, which are summarized in the figure on page 3. Over-all there was no difference in infection rates between the vaccine and placebo arms during the trial. But in the 314 African-American volunteers, 9 of 111 placebo recipients (8.1%) became infected, compared with 4 of 203 (2%) vaccinees. From these numbers, VaxGen initially reported 78.3% efficacy in this subgroup, with a confidence interval (CI) of 29-93% and a “p-value” <0.02—meaning that there is less than a 2% probability that these results are due purely to chance. Neither the Asian or mixed race subgroups (73 and 111 volunteers, respectively) gave statistically significant results, but when all 3 groups were combined, VaxGen calculated an efficacy of 66.8% (CI 30-84%; p<0.01).
|
It was these confidence intervals and p-values, plus the pooling of disparate racial groups, that were challenged after the webcast. That’s because the more subgroups analyzed in any study, the more likely it becomes that a seemingly significant result can arise by pure chance. To correct for this, the analysis must include a statistical penalty based on the total number of subgroups examined—which VaxGen, despite initial statements to the contrary, apparently did not do.
According to statistician Steve Self (University of Washington, Seattle and HIV Vaccine Trials Network), even conservative assumptions about the number of subgroups they analyzed drop the lower CI boundaries below zero and increase the p-values, greatly reducing the significance of the race-based efficacy claim. But he doesn’t dismiss the findings entirely, saying that the data raise “interesting, intriguing hypotheses that are worth pursuing.”
Does gender matter?
Berman also presented a breakdown of infection rates by gender, showing a trend towards more favorable results in women. Although vaccines are traditionally seen as gender-neutral, recent evidence that a candidate vaccine against HSV-2 may work only in women have challenged this notion, especially for sexually-transmitted diseases (see article, page 5). For AIDSVAX®, while there were 4 infections among 93 women given placebo (4.3%), only 1/175 female vaccinees (0.6%) became infected; for men, the figures were 94/1586 and 190/3155 (5.9 versus 6%). However, the results were not statistically significant, given the small number of women (about 5% of the cohort).
While the low numbers of women and minority volunteers (and infections) make it difficult to nail down the significance of these trends, gender may play a role in what VaxGen has viewed as race-based. Although Berman did not show gender data on the African-American subgroup (which was nearly 50% women), working back from VaxGen’s numbers indicates that 4/53, or 7.7% of black women given placebo became infected, compared with 0/93 vaccinees; for black men, it was 5/58 (8.6%) and 4/110 (3.6%). Adding to the uncertainty, the male-female differences could also reflect anal versus vaginal routes of transmission. In one clear lesson from the trial, this dilemma highlights the need to ensure that future cohorts are broadly representative of the wider population.
Antibody levels, HIV strain and protection
Searching for a possible biological explanation of race- (or gender)-based efficacy, Berman presented data on antibody titers in a small subset of the cohort. The studies measured both binding and neutralizing antibodies (NAb) to the vaccine’s lab-adapted HIV-MN strain, but not to GNE8, the second strain. GNE8 was isolated from an infected vaccinee in an earlier trial of AIDSVAX® (made only with the MN strain) and was later incorporated into the vaccine so as to broaden its range.
Overall, these data show modest trends in the “right” direction, but without answers yet on their statistical significance. NAb titers in uninfected white males given vaccine (124-139 men) were up to 30% lower than in vaccinated African-Americans (49-53 men); women had about 2-2.5-fold higher titers than men (comparing 67-82 women to 200 men).
Turning to studies of HIV strains in infected volunteers, Berman discussed whether AIDSVAX® may have blocked infection by viruses with gp120 identical to the vaccine, while allowing transmission of more divergent isolates. This “sieve analysis,” done by Peter Gilbert (University of Washington), was based on a 6 amino acid sequence in the V3 loop of both MN and GNE8 (although the sequences flanking this region differ between the two strains, according to Berman). Looking at volunteers from minority racial groups, the data showed that fewer vaccinees than placebo recipients were infected with strains matching the vaccine in this region (about 55 versus 30%, with p=0.0016). In contrast, white volunteers showed no differences in viral strains between vaccine and placebo groups.
These early data sets—which Berman says will take 6-12 months to complete—leave several issues unresolved. For example, since lab-adapted strains are far more neutralization-sensitive than primary ones, the MN neutralization data say little about whether AIDSVAX®-induced NAbs can block primary strains. Berman’s response is that conventional neutralization assays “do not reflect physiological conditions for antibodies directed against gp120,” and he rejects the notion that these data would shed light on whether AIDSVAX® is protective. However, results of passive antibody experiments in the monkey SIV model lend strong support to the predictive value of such assays (see IAVI Report, Dec 2002-Jan 2003).
A related question is the relevance of the region used for sieving, which is usually hidden from NAbs in primary isolates and therefore “an unlikely target for neutralization” of these strains, says antibody expert David Montefiori (Duke University). And, while the observed sieving is consistent with immune pressure from the vaccine, Montefiori asks whether there might be other explanations. For example, he speculates, “since the V3 loop is important in tropism, could strains with different V3 loops be more or less likely to transmit in different racial groups?”
After Banff: what’s next for AIDSVAX?
While at this point the data yield no solid evidence for protection in any subgroup, the question facing the vaccine community is whether they clearly exclude it—and, if not, whether further trials in humans may be warranted. But with VaxGen unable to fund such studies, says spokesman Lance Ignon, the onus has now shifted to NIH. On 23 April, the National Institute for Allergy and Infectious Diseases (NIAID) convened a meeting of outside HIV experts and key stakeholders with VaxGen scientists and collaborators to review the trial data. In a brief statement issued afterwards, NIAID said it would proceed with an independent analysis, leading to a decision on whether government funding for further development of the vaccine is justified. This process, say insiders speaking off the record, reflects a sense that the data on hand do not definitively refute VaxGen’s claim.
Additional analyses could also prove useful. One informative direction would be a sieve analysis over a longer region, ideally the full gp120—for which sequence data is available from 336 of 368 infections in the trial. (This collection—the largest set of sequences on newly-transmitted isolates—is “invaluable,” says Bette Korber.) Other studies might probe the biological activity of NAbs, for instance asking whether NAbs from vaccinees neutralize strains from infected placebo recipients (i.e., “un-sieved” strains) better than those from other infected vaccinees.
Another important issue is infection clusters—especially the 4 infections among placebo recipients at a single site in Chicago, on which the race and gender trends hinge. (This site enrolled one-third of all the trial’s women, and most were African-American; see article. The key question is whether these infections represent a statistical blip or non-vaccine factor, such as a social network among these volunteers—an idea made more plausible by the finding that 3 (and possibly all 4) women were infected by the same man, says site coordinator Parrie Graham. But she adds that these women are extreme loners leading marginalized lives, and that the transmitting male (involved in the local drug scene) is equally likely to have had sexual partners among the vaccinated volunteers. Continued monitoring of new infections in these and other volunteers in the subgroups of interest—even without the biannual vaccine boosts—might be one way to get more concrete answers.
Final data from a 2,500-person IDU study of AIDSVAX® in Thailand is expected late this year.
------------
*Patricia Kahn is editor of the IAVI Report.
With reporting by Mark Boaz.
| Copyright Information | Site map |