| AIDScience Vol. 2, No. 24, 6 December 2002 |
 |
| The need to understand vaccine demand |
| Why plans to deliver AIDS vaccines are on agendas today |
| by Emily Bass* |
| From the IAVI Report, the newsletter of the International AIDS Vaccine Initiative. Address correspondence to: ebass@iavi.org. Reprinted with permission from the IAVI Report. |
Given the scale of the AIDS epidemic and the limits of existing prevention technologies, demand for an AIDS vaccine can seem like a given. After all, who wouldn’t want an AIDS vaccine? Similarly, with immediate scientific challenges to overcome, plans for manufacturing an AIDS vaccine may seem like a distant concern.
But a chorus of voices, including veterans of other vaccine campaigns as well as AIDS vaccine advocates, warns that neither the science nor the supply-and-demand research can be shifted to the back burner. “I tell basic scientists that finding an AIDS vaccine is easy, compared with delivery,” says José Esparza, head of the WHO-UNAIDS Joint Vaccine Programme.
“There’s a belief that 'if you build it, they will come,’” says Mark Miller, who directs international epidemiology and population studies at the National Institutes of Health Fogarty International Center (Bethesda). “We know that this is just not the case.” Miller has tracked the slow uptake of hepatitis B (HB) and Haemophilis influenzae type B (HiB) vaccines, both approved in the last twenty-five years.
Instead, say Miller and others, vaccine stakeholders must plan ahead and gather information on a wide range of topics that fall under the broad rubric of need and demand. These familiar terms have specific meanings in the public health lexicon: Demand refers to the number of doses that a country can deliver using existing infrastructure, and the number of people who are willing to be immunized. Need refers to the maximum number of people who could benefit from the vaccine, based on disease burden and the size of at-risk populations.
Experts seeking to understand need and demand ask deceptively simple questions, like how much vaccine the world actually needs: How much can be made, and how many people are likely to come forward for immunization.
While these queries are common to all vaccines, others will be faced for the first time by the AIDS vaccine field: What will the demand be for a vaccine that offers only partial protection (a likely scenario for a first-generation AIDS vaccine)? How can vaccines for a highly-stigmatized disease be delivered safely and swiftly to adults, who are not the primary target of existing immunization programs? If the world is to avoid delays in delivery, these questions must be addressed long before a vaccine is licensed. “We’ve only started to scratch the surface” of these issues, says Jane Rowley, a health economist and IAVI advisor.
A glimpse of what’s at stake could come soon. In early 2003, VaxGen is expected to release results from the first of its two Phase III AIDS vaccine trials. If the results are favorable, the world could have the first partially-effective AIDS vaccine—and a host of decisions about licensing and distribution—on its hands. Should demand outstrip supply, the world will need fast, reliable directives on where the vaccine will have the most impact and how it can be delivered rapidly to different populations.
Vaccine properties such as route and immunization schedule are known for the VaxGen candidate, making it easier to query countries, communities and individuals about anticipated demand. But most of today’s assessments concern products that don’t yet exist, and where it’s unclear what properties they will have.
A survey of vaccine delivery in the last century underscores the urgent need for advance planning. Yellow fever vaccine, available since 1937, is used in less than one-third of the countries where the disease is endemic. Hepatitis B vaccine was licensed in 1981 but reaches less than half of the world’s children in routine schedules. Several factors account for this delay. A study by Mark Miller and colleagues found that vaccine cost, delivery infrastructure and burden of disease were the strongest predictors of whether or not HB and HiB were added to childhood immunization programs. Such studies—and the difficulties faced by global vaccine procurers from UNICEF to the Global Alliance for Vaccines and Immunization (GAVI)—reveal the problem in stark relief: Without planning and action, vaccine need will far exceed vaccine demand.
Opening acts
There are many ways to approach demand assessments. Surveying this wide and varied field, José Esparza reaches for the parable of the blind man and the elephant, in which each man describes a wholly different beast depending on where he stands in relation to it. “Immunology people will say that the most important determinant of AIDS vaccine use is efficacy,” he says. “Policy people will say that it is cost.”
Studies to date (see References) offer a variety of perspectives on the elephant. In 2000, Esparza’s group, along with IAVI, co-sponsored four regional consultations (in Africa, Latin America, Eastern Europe and Asia) that gathered representatives from government, NGOs, and research institutions to discuss public sector demand for AIDS vaccines of different efficacy levels. After being briefed on the nature of partially-effective vaccines (see IAVI Report, July-September 2002), participants used epidemiological and public health data from one country as the basis for assessing regional need and demand for two vaccines: one of low to moderate efficacy (30-50%), the other with high efficacy (80-90%).
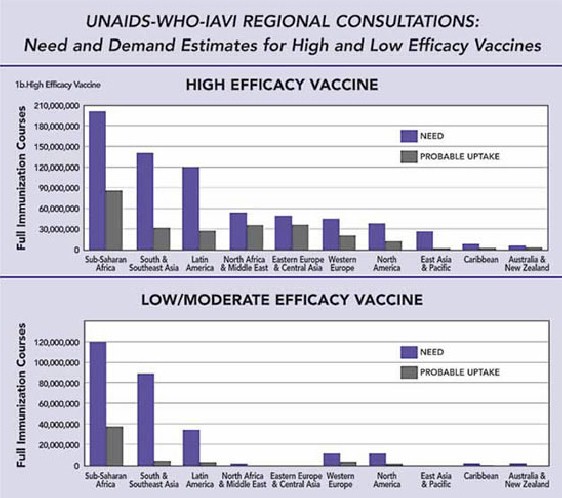
Source: WHO-UNAIDS, Global Need and Current Delivery Capacity for Future HIV Vaccines, 2002 (XIVth International AIDS Conference, Abs. #WeOrD1297)
Need and demand are estimated using different types of data. Models of need draw on epidemic conditions, incidence and prevalence data, along with assumptions about how long vaccine protection will last. Demand estimates draw on actual vaccine usage, as well as data on accessibility (the number of people who could reasonably be vaccinated by existing services), and acceptability (the willingness of individuals, health ministries, and other entities to purchase and use vaccines with a given set of properties).
Ultimately, the consultations found striking gaps between need and demand (see figure, below). The groups came up with an estimated global need of 260 million immunization courses for a low-to-moderate efficacy vaccine, but a demand for only 49 million. For a high-efficacy vaccine, need was estimated at 690 million courses and demand at 260 million.
While these figures throw the gap between need and demand into stark relief, veterans of the field say that these discussions, which did not draw on recent modeling work, probably underestimated the actual numbers. Esparza agrees, emphasizing that these discussions were “more qualitative than quantitative.” One striking example came from Russia and Eastern Europe, where AIDS incidence has increased by 1300% between 1996 and 2001—yet participants from the region said that a low-efficacy vaccine might not be used at all. The concern voiced by health authorities was that a low-efficacy vaccine could do more harm than good by creating a false sense of security in vaccinees.
So far, a handful of studies have looked at whether or not behavior change could negate (or improve) the positive effect of a vaccine. One recent paper came from the Harvard School of Public Health. Using data from a Thai cohort of intravenous drug users, they modeled the long-term (40-year) impact of vaccines with 30%, 75% or 90% efficacy, delivered to 50% of the cohort. Their findings: In the absence of behavior change, both vaccines reduced prevalence. For the higher-efficacy vaccine, a 50% increase in risky behavior had only a minimal effect on long-term prevalence. Looking further, they found that even if 50% of vaccinees given the low-efficacy vaccine increased risk behavior, prevalence did not increase over forty years.
Of course, the world is unlikely to launch huge vaccination campaigns that may have only marginal effects on long-term prevalence. To maximize the effect of low-efficacy vaccines, Esparza says that countries should prepare to couple immunization campaigns with robust prevention and care services. This means that, at least in the short term, vaccines should not be seen as potential cost-saving measures.
Countries and vaccine stakeholders will also need to consider immunization strategies that seem counter-intuitive at first glance. Roy Anderson and colleagues at Imperial College (London) have created models which suggest that targeting high-risk individuals is not always the best use of low-efficacy vaccines. In an early epidemic, a targeted strategy may contain HIV spread. However, in a mature epidemic, many people from high-risk groups will already be infected by the time a vaccine program reached them. In this case, a universal immunization strategy would be more effective.
What industry needs
Need and demand estimates are also crucial to private sector decision-making about advancing products from the laboratory to clinical trials and then to the marketplace. At early stages, trial planners rely on models that help set the minimum efficacy threshold a trial should be powered to detect. Then, as products move into trials, questions about demand come to the fore. How many of the countries that need vaccine will be able to deliver it, and how many doses will they need? Perhaps the most important question: Is there sufficient manufacturing capacity and technology to meet global demand?
Building industrial capacity for vaccine production typically requires four to five years lead-time, hundreds of millions of dollars and extensive regulatory oversight. Making matters worse, decisions about building production plants must be made before the results of Phase III trials are known (as VaxGen has done) if major delays between licensing and wide-scale availability are to be avoided. To help hedge its bets, VaxGen has designed its new manufacturing facilities (in Seoul, South Korea, and San Francisco, USA) to be multi-purpose, suitable for producing a range of human therapeutic proteins.
None of this is new terrain for pharmaceutical giants like Merck and GlaxoSmithKline. “Industry always does a lot of marketing projection and demand work for its own purposes, but this information is usually regarded as commercially sensitive and not publicly available,” says Saul Walker, IAVI’s European Policy Coordinator. But since vaccines, including AIDS vaccines, are needed most in countries with little ability to pay, public sector groups also need information on demand, both to encourage investment in vaccine development and to inform plans for delivery infrastructure and financing mechanisms.
Increasing infrastructure
While making, purchasing and bringing vaccines to developing countries is a daunting task, many experts say that the real challenges start at the airport, after the vials have been unloaded for distribution throughout the country. It’s here that the issue of uptake—demand with a reality check—comes into play. Are there sufficient refrigerators, trucks, syringes and syringe disposal facilities for the vaccine dispensaries? Are there trained personnel at these dispensaries? Is there capacity for community outreach and for follow-up to individuals who do not complete their immunization course? In short, is the necessary infrastructure in place? If the answer is no, then it will not matter whether a country has an explosive epidemic or an early one that could be stopped with a relatively small-scale immunization campaign. Without infrastructure, there is an unbridgeable chasm between need and demand.
Given the singular level of global advocacy around AIDS, stakeholders may be able to mobilize for improved infrastructure and the funds to build it. But to succeed, they must figure out what delivery infrastructure is needed for vaccines with different properties so that steps to build it can begin early; just as with manufacturing capacity, delivery capacity cannot be built overnight once a vaccine is licensed.
Even countries that seem prepared for delivery may need extra support. This is one lesson GAVI learned in 2000 when it adopted DTP coverage (defined as a full, three-dose cycle of diptheria, tetanus and pertussis vaccine given to children under age one) as its indicator of whether a country has adequate infrastructure to qualify for funding. Two years later, preliminary results reveal a patchy infrastructure in many countries, with cold chains, safe syringe disposal, and trained personnel lacking. GAVI has since opened a new funding “window” to improve delivery infrastructure.
The GAVI experience gives some sense of the road ahead—but it could be an even bumpier ride for AIDS vaccines, which cannot rely on DTP coverage (which reflects the ability to deliver vaccines to infants) as the sole “proxy” for estimating capacity. Instead, new infrastructure surrogates for AIDS vaccines will have to be developed under different sets of assumptions about vaccine properties and use, such as whether they need refrigeration, the number and route of immunizations, and the population the vaccine is approved for—which is likely to be an adult population, at least initially. Proxies will also depend on who among the adult population is being targeted for vaccination.
Miller says that voluntary counseling and testing sites may be a reasonable proxy for AIDS vaccines, and that, by expanding these services, countries can lay the groundwork for eventual delivery.
But even with a healthy infrastructure and stacks of impact studies, the best laid plans will still go awry if people refuse immunizations, or do not come forward. This could happen for many reasons, including rumors and misinformation, mistrust of the medical establishment or the vaccine itself. Stigma could also play a role—especially in immunization campaigns targeting high-risk groups.
The world learned this lesson with hepatitis B vaccine. When it was licensed, experts recommended universal infant immunization in some areas, and targeted immunization of high-risk groups in others. However, stigmatization of the disease (and, by extension, its vaccine) led to low numbers of high-risk people coming forward to be vaccinated, so the targeted strategy was abandoned in favor of universal infant immunization. Similarly, uptake of treatments that reduce mother-to-child transmission of HIV has been lower than expected in some areas of the developing world, in part because many women are reluctant to learn their HIV status or discuss it with their partners.
Future actions
The good news is that the demand “elephant” is beginning to get more attention from a variety of perspectives. With the imminent announcement of VaxGen’s trial results, the WHO-UNAIDS Vaccine Programme is holding a meeting (20-21 November) on the potential uses of partially-effective vaccines and the specific questions that could be raised by the VaxGen data. José Esparza and Mark Miller have also mapped out a comprehensive set of actions addressing facts of demand that will be pursued in the coming years.
At IAVI, a new Demand Project will help fill in some of the gaps by collecting background data to inform detailed projections of need and demand. This includes infrastructure needs for delivering health commodities to adults, and in-country approval processes for new products licensed by global agencies. The project will also support further modeling work and analyses of factors influencing decisions on vaccine use.
But estimating demand is an evolving task that won’t end when the field has completed this (or any other) set of studies, or derived a particular set of numbers; rather, it will continue to shift along with the epidemic and the world’s response to it. Forward-looking studies are also needed to track the impact of more widely available antiretroviral treatment on the capacity to deliver AIDS vaccines.
One such analysis is an ongoing project at Johns Hopkins and the Rakai Project (Uganda) that uses epidemiological data from Rakai to explore the potential impact of vaccine and treatment strategies on HIV prevalence. Increases in access to antiretrovirals (ARVs) should not be seen as reducing the need for an AIDS vaccine, says Mark Miller. Instead, the two may work in tandem, with ARVs increasing countries’ interest in vaccines by setting a precedent for spending on more complex, costly interventions. “If major treatment options are implemented, this will only make prevention with an effective vaccine more valuable,” he says.
References
Existing AIDS vaccine demand and related studies in the public domain**
PUBLIC SECTOR DEMAND
Bishai, D. et al. Algorithms
for the Purchase of an AIDS Vaccine
Working Paper #2321 (2000) from the World Bank Health and
Population, Fertility and HIV/AIDS Working Group available at:
http://econ.worldbank.org/docs/1072.pdf
Two mathematical models of decision-making on purchase of
hypothetical vaccine: one employing health sector priorities
(minimizing government health spending on HIV/AIDS); and one based
on societal priorities (minimizing impact of HIV/AIDS on health
spending and GDP
Bishai, D. et al. Modeling
the Economic Benefits of an AIDS Vaccine
Vaccine
20:526;2001
Global demand estimates based on cost-benefit analyses
Esparza J. et al. Global
and Regional Estimates of Need and Probable Uptake for HIV/AIDS
Preventive Vaccines..Vaccine 2002 (in press)
Regional experts indicate likely policies for use, which are
translated into aggregated public health needs for vaccine.
Estimates made for vaccines of low and high efficacy
Tangcharoensathien, V. et
al. The Potential Demand for an AIDS Vaccine in Thailand,
Health
Policy
57:111;2001
Demand estimates based on targeted delivery to 8 risk groups,
calculating cost/savings per HIV infection averted
INDIVIDUAL WILLINGNESS TO PAY
Suraratdecha, C. et al.
The Demand for an HIV/AIDS Vaccine: Does Risk Matter?
PowerPoint Presentation from 14th International AIDS Conference,
Barcelona 2002 available at:
http://www.iaen.org/files.cgi/7420_chutima.pdf
Estimates of individual (high risk groups and general population) willingness to pay for vaccines with 50 or 95 percent efficacy
Whittington, et al. Private
Demand for an HIV/AIDS Vaccine: Evidence from Guadelejara, Mexico Vaccine
20:2585;2002
Private demand estimates based on willingness of individuals to pay
for AIDS vaccines
IMPACT STUDIES
Bogard, E. et al. The
Impact of a Partially Effective HIV Vaccine on a Population of
Intravenous Drug Users in Bangkok, Thailand: A Dynamic Model
JAIDS
29:132;2002
Models impact (on 40 year prevalence rates) of 30, 75, and 90
percent efficacious vaccines in a cohort of Thai IV drug-users
Longini, I., et al. Model-based
Estimation of Vaccine Effect from Community Vaccine Trials. Stat
Med
21:481;2002
Estimates of epidemiological and economic impact of intervention
based on a “Thailand-like” situation
Stover, J., et al. The Epidemiological Impact of an HIV/AIDS Vaccine in Developing Countries (2002) Working Paper #281 from the World Bank Development Research Group available at: http://www.policyproject.com/pubs/countryreports/Vaccine_World_Bank_article.pdf
Three models for impact of partially-effective vaccines based on epidemiological data from rural Zimbabwe, Kampala, Uganda, and Bangkok, Thailand
OTHER
Miller, M. et al. A
Model to Estimate the Probability of Hepatitis B- and Haemophilis
influenzae type b-vaccine Uptake into National Vaccination Programs.
Vaccine
18: 2223;2000
Analysis of determining factors in countries’ decision to include
two new vaccines in existing childhood immunization programs
Watts, C. et al. The
Public Health Impact of Microbicides: Model Projections PowerPoint
presentation (and other documents and tools related to prevention,
treatment and microbicide impact) available at:
http://www.hivtools.lshtm.ac.uk/
Model of impact of partially effective microbicides
**Compiled by Tom Nassim (IAVI consultant), Yvette Madrid (IAVI consultant) and Saul Walker (European Policy Coordinator, IAVI).
------------
*Emily Bass is senior writer of the IAVI Report. Additional reporting by Tom Nassim, a graduate student at the Harvard School of Business and an IAVI consultant.