| AIDScience Vol. 3, No. 19, 2003 |
| Recent trends in HIV prevalence among pregnant women in sub-Saharan Africa |
| By E. Asamoah-Odei1, G. Asiimwe-Okiror2, J. M. Garcia Calleja3, and J. T. Boerma3 |
| 1World Health Organization, Regional Office for Africa, Harare, Zimbabwe 2Consultant, Harare, Zimbabwe 3World Health Organization, Geneva, Switzerland |
| Address correspondence to: boermat@who.int |
Abstract
The HIV/AIDS epidemic in sub-Saharan Africa accounts for more than two-thirds of the world’s HIV infections, and is commonly referred to as a one-Africa epidemic. Recent trends based on surveillance of pregnant women attending antenatal clinics, however, clearly show that, from both the epidemiological and programmatic perspectives, it is no longer appropriate to consider the existence of such epidemic. There are huge differences in HIV prevalence between countries, striking sub-regional patterns can be observed and the gap between the sub-regions appears to be widening. The extent to which southern Africa is affected by the epidemic will have very different implications for prevention, care and treatment, and will impact mitigation programs. These implications are likely to be different from those in eastern Africa, where HIV prevalence appears to be two-thirds lower with evidence of a modest decline, or to Western Africa where HIV prevalence is roughly one-fifth of that observed in southern Africa and no rapid growth is occurring.
Introduction
With more than two-thirds of global HIV infections, sub-Saharan Africa is by far the most affected region of the world. At the end of 2002, it was estimated that about 29 million people were living with HIV infection in this region, with nearly 9% of adults between 15 and 49 years old infected (1). The estimates of the size of the epidemic are based on data generated by national HIV surveillance systems in different countries in previous years. Sentinel surveillance systems in sub-Saharan Africa primarily rely on data from pregnant women attending prenatal clinics. Such data not only form the basis for national estimates of the size of the epidemic (2), but also, more importantly, are the main source of data on the course of the epidemic in this region.
This paper focuses on recent trends in HIV prevalence among women attending prenatal clinics, using surveillance data reported by national programs in countries in the African region of the World Health Organization (WHO) (3). The 2002 round of surveillance included over 600 prenatal clinics and over 200,000 women, which provides a unique opportunity to assess recent trends in HIV prevalence within countries and sub-regions of sub-Saharan Africa.
Methods
In recent years, HIV surveillance systems have increased the number of sentinel clinics in many countries. Others have changed the surveillance system design or changed the location of the sentinel clinics, which may affect trends. Since the focus of this assessment is to examine trends, it limits itself to the same clinics with data over multiple years. The median of HIV prevalence data of prenatal clinics is used as a summary measure.
The data for the analysis are derived from the HIV surveillance country reports for 2002 from 24 countries in WHO African Region. In cases when no 2002 report was available, the 2001 reports were used (Ethiopia, Gabon, Gambia, Guinea, Malawi, Nigeria, Uganda, Zimbabwe) or in a few countries the 2000 reports (Niger and Togo).
Typically, sentinel prenatal clinics are surveyed for a period of about 6 weeks in a year, when samples from 300 to 500 women are collected. Unlinked anonymous HIV testing is conducted on residual blood from samples taken for other purposes (usually syphilis testing). Most countries have a quality control component in place, although the reporting on the results of the quality control is irregular. Different approaches are used to select the prenatal clinics. Most countries have selected one or two sites located in the majority of the nation’s provinces or regions, often one site in the regional capital and a second site in a semi-urban area within the same region or province. South Africa is the only country that uses probability proportional to size sampling to select sentinel sites from a listing of public prenatal clinics with client volume.
Twenty two countries have sufficient data to assess the trend for the 1997 to 2002 period, including over 300 prenatal clinics in 21 countries plus South Africa’s sampling system with about 400 clinics. Only prenatal clinics that have at least one measurement in each of the three two year periods (1997-1998, 1999-2000 and 2001-2002) are included. Most clinics with data for multiple years are located in urban or semi-urban areas.
The United Nations General Assembly Special Session (UNGASS) on HIV/AIDS declaration and the Millennium Development Goals (MDG) have set the goal of reducing new infection rates among young people (4). HIV prevalence among pregnant women between 15 and 24 years old is used as an indicator of the new infection rate in countries with a generalized epidemic. Several studies have shown that a decrease in HIV prevalence starts with a decline in the prevalence among young pregnant women (5, 6). Prevalence among pregnant women between 15 and 19 years of age is a relatively unstable indicator of trends in HIV incidence and prevalence and, therefore, prevalence among pregnant women between 15 and 24 years old is a preferred measure (7). An increasing number of countries now present HIV prevalence among pregnant women by age.
Results
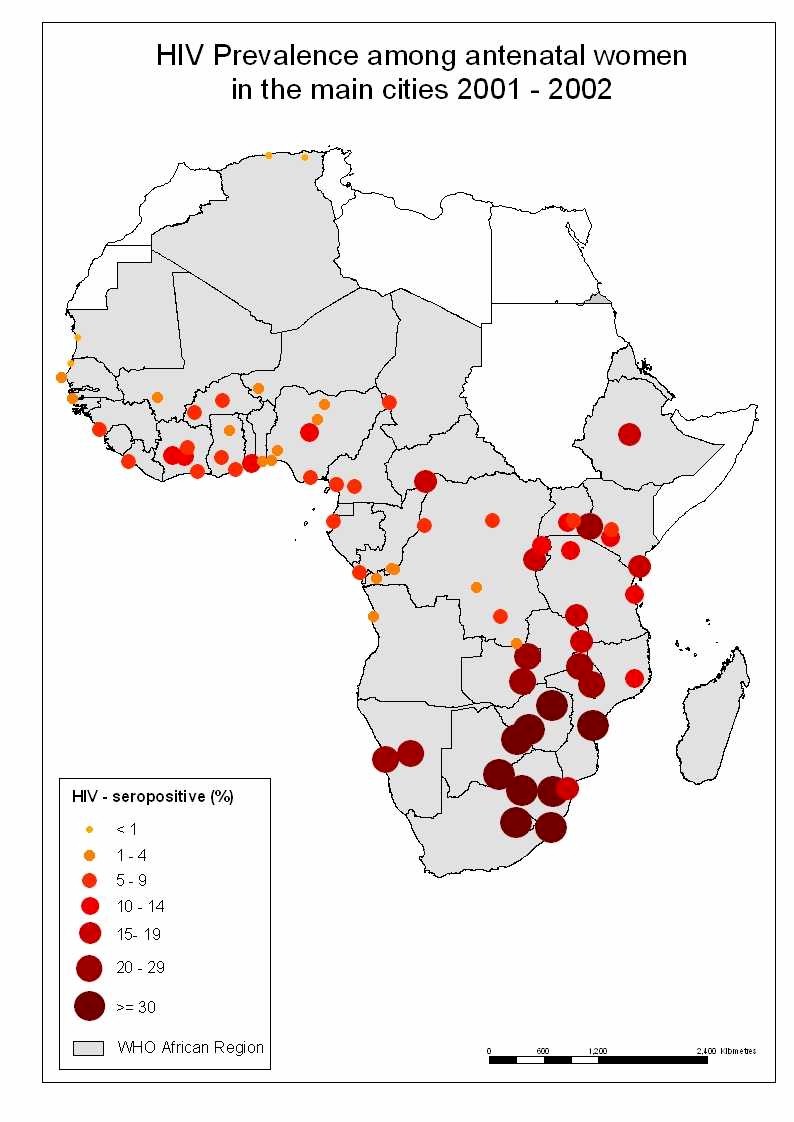 |
| Figure 1. [Enlarge] HIV prevalence among pregnant women in main cities, 2001-2002. |
There was a major variation in HIV prevalence among pregnant women attending prenatal clinics between capitals, major cities and large towns within the African region in 2001-2002 (Figure 1). In southern Africa most prenatal clinics in cities and large towns had levels of HIV prevalence over 20%, with the exception of Maputo and Nampula in Mozambique, Luanda in Angola, and Mzuzu in Malawi. In eastern Africa, HIV prevalence in prenatal clinics in cities ranged from 10 to 17%, with only Jinja in Uganda below 10%. Out of 33 cities and large towns in western and central Africa, the most recent data on HIV prevalence among pregnant women exceeded 10% only in Abuja, Nigeria, in Daloa and Yamoussoukro, Côte d’Ivoire, in Yaounde, Cameroon, and in Bangui, Central African Republic.
The trend in HIV prevalence in the same prenatal clinics indicates that the large gap in HIV prevalence between sub-regions of Africa is not reducing but widening (Table 1). The median HIV prevalence in the seven countries in southern Africa having data for all three two-year periods increased considerably from 20% in 1997-98 to 26% in 2001-2002 (Table 1). Data from eastern Africa suggest that there has been a decline of HIV prevalence among pregnant women. Data for all three two-year period were not available in countries in Central Africa, but it is possible that an increase in prevalence exists. In western Africa, where HIV prevalence in urban clinics was often in the order of 5%, there was a modest decrease in some countries and a gradual increase in others, with no clear overall increase. The median HIV prevalence of 67 prenatal clinics surveyed in 1999 and 2001 in Nigeria, the most populous country in the region, increased from 4.3% to 5.0%.
Table 1. Trends in HIV prevalence by country in the same prenatal clinics, with regional medians for countries with all three periods.
|
Data from prenatal clinics in major cities were available for most of the 1990s. Figure 2 presents the trend in HIV prevalence in cities by sub-region for six two-year periods since the early 1990s. In seven major cities in southern Africa (including Gauteng province as an approximation for Johannesburg), there has been a continuing increase throughout the last decade. HIV prevalence in southern African cities exceeded prevalence in eastern African cities in the mid 1990s and is currently twice as high. The median HIV prevalence for eastern African cities has declined gradually during the last three two-year periods. This decline is most dramatic and most consistent in Kampala, Uganda, but other cities in eastern Africa have also shown drops in HIV prevalence, notably in Bujumbura, Burundi, in Kigali, Rwanda and in Addis Ababa, Ethiopia.
Data from four central African capital cities suggest an increasing HIV prevalence, but the data have to be interpreted carefully. In western Africa, HIV prevalence levels in seven capital or major cities have remained fairly constant during the mid and late 1990s. Recent data suggest a modest decline, which is due to decreasing prevalence in Abidjan, Cote d’Ivoire, in Cotonou, Benin, in Lagos, Nigeria, and in Ouagadougou, Burkina Faso. Abidjan has recorded one of the highest levels of HIV prevalence in western Africa throughout the 1990s. In 2002, Abidjan reported its lowest HIV prevalence among pregnant women in a decade (7.4%).
Several countries provided data on HIV prevalence among pregnant women by age in the surveillance report, but only a few countries have done so in the past. Figure 3 presents a summary of HIV trends among young pregnant women attending the same surveillance prenatal clinics in six countries with trend data during 1997-2002. At the high end, HIV prevalence among pregnant women between 15 and 24 years old has increased to nearly 40% in Swaziland. At the low end, two western African countries had HIV prevalence well below 5%. There was little evidence of a significant decline.
Discussion
 |
| Figure 2. Median of HIV prevalence (%) in capital cities, by sub-region (number of capital cities), 1991-02. |
There is an increasing volume of data on the spread of HIV in sub-Saharan Africa. Many countries are improving and expanding their prenatal clinic-based surveillance systems. This includes expansion of the system into more rural areas. Also, an increasing number of countries are conducting population-based surveys with HIV testing (3, 8).
The trend in HIV prevalence in the same prenatal clinics in recent years suggest that the epidemic growth has leveled off in the late 1990s in most countries, but there is no convincing evidence of a broad decline. Because several countries are getting better data on rural populations, HIV estimates will be adjusted downward in the near future. This should not be confused with a decline of HIV prevalence and incidence.
The trends in HIV prevalence in observed in the same sites suggest that the large differences in HIV prevalence by sub-region are not temporary and that the gap between the sub-regions is widening. Trends by sub-region indicate a continuing increase in southern Africa, where levels are extremely high with at least one-fourth of pregnant women infected with HIV in most countries. In central Africa, data availability is poor but HIV prevalence appears to be increasing. In eastern Africa, HIV prevalence is decreasing and this decrease occurred in urban and semi-urban sentinel sites in Burundi, Ethiopia, Kenya, Rwanda and Uganda. In western African countries, where prevalence is generally about one-fifth of that in southern Africa, a mix of modest decreases and increases can be observed. Data on HIV prevalence among young pregnant women between 15 and 24 years old are a marker of a decline in HIV incidence, but only a few countries have presented such data in previous years to allow an assessment of trends over time. There is a need to further standardize the reporting of HIV prevalence among young prenatal attendees in the same way that has been done for pregnant women of all ages attending prenatal clinics.
 |
| Figure 3. Median HIV prevalence (%) among the same prenatal clinics for women 15-24 years, selected countries, 1997-02. |
Some biases need to be considered when interpreting the trend in HIV prevalence data. Focusing on the same prenatal clinics only eliminated an important bias. Changes in patterns of prenatal care utilization are unlikely to have an important effect on the trend. There are isolated clinics in which a large change in HIV prevalence could be attributed to abrupt economic changes (such as the collapse of the tourism industry), but overall this should have a small effect on the trends in all clinics combined. The extent to which HIV trends among pregnant women are representative of trends in the general adult population may vary. An important factor is the high level of prenatal care attendance in most countries. Prenatal care attendance exceeded 75% in nearly three-quarters of the countries of the region.
A second bias could be related to HIV testing strategies. Overall, no major changes appear to have taken place in testing strategies, which recommend a single HIV test for surveillance in countries with HIV prevalence of 10% or higher and a screening and confirmatory test in countries with HIV prevalence below 10% (9). Some countries report the results of the quality control testing, but there is a need to improve these reports.
HIV prevalence trends among pregnant women can also be affected by changes in fertility, especially if caused by HIV (10, 11, 12). In particular, if the fertility-reducing effect of HIV were associated with the duration of infection (13), a decline in HIV prevalence would be observed in any maturing epidemic, once the mean duration of infection in the population became longer. There is little empirical evidence of such changes, and for now it can be assumed that HIV prevalence trends are only moderately affected by the HIV-fertility association.
Lastly, the majority of prenatal clinics with trend data are located in urban areas. Much less is known about HIV prevalence trends among rural pregnant women. Recent data from prenatal clinics and population-based surveys indicate much lower prevalence in rural population (3). Urban-rural differences tend to be smaller in southern Africa than elsewhere in Africa, which further accentuates the difference between the two sub-regions.
In countries with widespread epidemics, HIV prevalence trends among pregnant women are considered indicative of trends in the general adult population (2). In countries with less severe epidemics (referred to as concentrated or low level epidemics) tracking HIV prevalence among risk populations is the mainstay of surveillance. Only a few countries in Africa have established a system of regular HIV surveillance among sex workers. The best example is Senegal where surveillance among female sex workers has been conducted in several urban areas on a regular basis since the late 1980s. HIV prevalence among sex workers in Dakar has remained at levels just under 20% in recent years. In Abidjan, Côte d’Ivoire, and Cotonou, Benin, declining HIV prevalence has been observed among sex workers during the 1990s (14,15).
HIV surveillance in the same prenatal clinics will continue to be important for the monitoring of trends. At the same time, surveillance systems will have to expand in several directions. Including multiple smaller clinics in rural areas can improve coverage of rural populations. The scaling up of HIV programs, such as prevention of mother to child transmission and voluntary testing and counselling, is both a challenge and an opportunity for current surveillance systems. Population-based surveys with HIV data collection can provide important additional information on the status of the epidemic, provided the surveys are of high quality and have satisfactory response rates (8). Population-based surveys are not intended to replace continuous sentinel surveillance system, but constitute a valuable addition primarily because they provide data on men, non-pregnant women and rural populations.
The trends in HIV prevalence among pregnant women attending the same prenatal clinics in recent years suggest that the epidemic growth has leveled off in the late 1990s, but there is no decline. There are huge differences in HIV prevalence between countries and clear sub-regional patterns can be observed. The gap between sub-regions appears to be widening. It is not appropriate to talk about a single epidemic in sub-Saharan Africa. From the epidemiological perspective, the extent to which southern Africa is affected by the epidemic will have very different implications for prevention, care and treatment, and will impact mitigation programs compared to other parts of sub-Saharan Africa.
References and notes
| 1. | “AIDS Epidemic update: December 2002”, (UNAIDS and WHO, Geneva, 2002). Available online |
| 2. | UNAIDS Reference Group on Estimates, Modelling and Projections, AIDS 16, W1 (2002). PubMed |
| 3. | "HIV/AIDS Epidemiological Surveillance Update for the WHO African Region 2002," (WHO Regional Office for Africa, Harare, 2003). Available online |
| 4. | “Monitoring the declaration of commitment on HIV/AIDS. Guidelines on construction of core indicators,” (UNAIDS, Geneva, 2002). Available online |
| 4. | G. Asiimwe-Okiror, et al., AIDS 11, 1757 (1997). PubMed |
| 6. | A. Tsegaye, et al., J. Acquir. Immune Defic. Syndr. 30, 359 (2002). PubMed |
| 7. | B. Zaba, J.T. Boerma, R.White, AIDS 14, 1633 (2000). PubMed |
| 8. | J.T. Boerma, P. Ghys, N. Walker, Lancet, in press. |
| 9. | "Guidelines for Using HIV Testing Technologies in Surveillance: Selection, Evaluation and Implementation," (UNAIDS and WHO, Geneva, 2002). Available online |
| 10. | E. Boisson, A. Nicoll, B. Zaba, L.C. Rodrigues, J. Acquir. Immune Defic. Syndr. 13, 434 (1996). PubMed |
| 11. | L.M. Lee, et al., Am. J. Epidemiol. 151, 1020 (2000). PubMed |
| 12. | S.C. Hunter, et al., J. Biosoc. Sci. 35, 189 (2003). PubMed |
| 13. | B. Zaba, S. Gregson, AIDS 12 (suppl. 1), S41 (1998). PubMed |
| 14. | M. Alary, et al., AIDS 16, 463 (2002). PubMed |
| 15. | P.D. Ghys, et al., AIDS 15, 1421 (2001). PubMed |
| Copyright © 2001 by The American Association for the Advancement of Science |